For many high-sensitivity users, a low-oxalate diet starts as a useful safety tool. But when symptoms persist despite careful restriction, the next question is not always “Which food do I remove next?”
The better question is:
Why is the oxalate threshold so narrow in the first place?
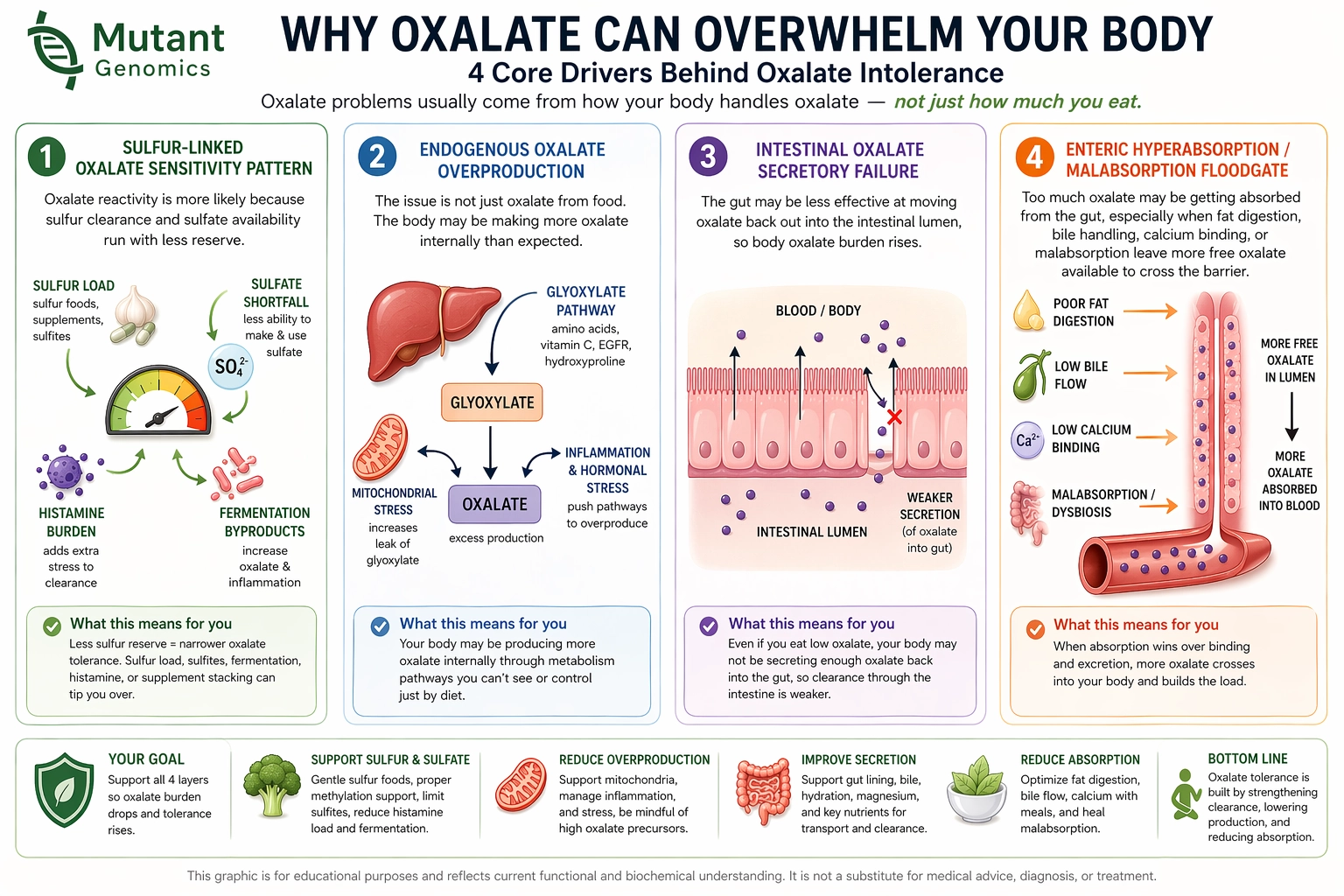
Mutant looks at four different biological patterns that can make oxalate burden feel larger than diet alone explains:
Each pattern points to a different protocol. The goal is not to force oxalate dumping, restore Oxalobacter, or rush oxalate reintroduction. The goal is to make the system more stable, reduce false signals, and identify which lane is actually worth supporting.
If a low-oxalate diet is not enough, the next step is not always more restriction. Oxalate stability depends on which biological driver is narrowing your threshold.
Oxalate sensitivity is often treated as a single problem: too much oxalate in the diet.
But many users do not fit that simple model. Some react even when intake is low. Some flare when sulfur load rises. Some worsen after high-fat meals. Some seem tied to constipation, gut instability, or poor stool form. Others may have internal production pressure that diet alone cannot explain.
Mutant separates these patterns so the user does not keep applying the wrong strategy.
A stricter food list may help in some cases, but it does not explain every oxalate pattern. The Mutant roadmap asks:
The answer changes the protocol.
This roadmap is about driver matching and protocol direction.
It is not:
It is designed to help users avoid the common trap of treating every oxalate issue the same way.
The first win is not “eating high oxalate again.”
The first win is:
a calmer baseline, fewer false flares, cleaner feedback, and a better-fitting next step.
The pattern:
Oxalate tolerance appears to narrow when sulfur load, sulfite pressure, or sulfur-handling bottlenecks are active.
This can show up when users react more strongly during periods of high sulfur foods, sulfur supplements, aggressive detox stacks, or increased sulfite burden.
What Mutant looks for:
A pattern where oxalate reactivity may be amplified by sulfur clearance pressure, reduced sulfate reserve, or sulfur-handling bottlenecks.
Protocol direction:
The protocol does not start by pushing sulfur harder.
It starts by lowering sulfur demand, reducing noisy inputs, using micro-dose molybdenum only when appropriate, avoiding sulfur overshoot, and rechecking whether Lane 1 becomes quieter.
Key idea:
Do not assume sulfur sensitivity means “add more sulfur.”
In this lane, the first goal is readability and stability.
The pattern:
Oxalate burden may be driven partly by internal production through glyoxylate-handling pathways rather than food intake alone.
This can fit when oxalate burden seems disproportionate to intake, especially after obvious enteric, export, vitamin C, hydration, and stone-risk confounders are separated by the platform.
What Mutant looks for:
A pattern involving glyoxylate-handling fragility, vitamin C exposure, B6/PLP dependency, and related metabolic pressure.
Protocol direction:
The protocol does not ask the user to keep sorting the source manually. The platform already does that.
The protocol focuses on:
Key idea:
This is not a high-dose B6 protocol.
It is an internal-production suspicion protocol that uses cleaner data before escalating.
The pattern:
Oxalate burden may rise because the intestine is less able to move oxalate from the body back into the gut for elimination.
This is different from absorbing too much oxalate from food. It is a possible “export lane” issue.
What Mutant looks for:
A pattern involving gut instability, stool rhythm, epithelial stress, mucus surface integrity, and intestinal oxalate export biology.
Protocol direction:
The protocol does not try to force oxalate dumping.
It focuses on:
Key idea:
The gut export lane cannot be read clearly when constipation, SIBO flares, dehydration, or unstable stool form are dominating the signal.
The pattern:
Oxalate burden may rise because the gut absorbs too much oxalate under malabsorption conditions.
This can happen when fat malabsorption, bile-acid disruption, or poor calcium binding leaves more free oxalate available in the gut.
What Mutant looks for:
A meal-linked pattern involving fat intolerance, loose or greasy stools, bile-flow clues, surgical history, IBD-like context, or poor binding margin.
Protocol direction:
The protocol focuses on:
Key idea:
This is not just “take calcium.”
The timing matters. Calcium works in the gut lumen when paired with the oxalate-containing meal.
Oxalate protocols often fail when the wrong mechanism is targeted.
For example:
The same symptom can have different upstream drivers.
That is why Mutant does not present one universal oxalate protocol.
It ranks the likely drivers and gives a protocol that matches the pattern.
See which oxalate driver appears most relevant to your pattern.
Mutant does not assume all oxalate sensitivity is dietary. It separates sulfur-linked sensitivity, internal production, intestinal export failure, and enteric hyperabsorption.
Your oxalate result is interpreted alongside related biological modules such as sulfur handling, glyoxylate metabolism, gut transport, fat digestion, mineral binding, and barrier stability.
Each driver points to a different protocol.
The goal is to avoid random stacking and help you start with the lane that best fits your profile.
The first objective is not to add more interventions.
The first objective is to reduce noise, stabilize the baseline, and make the next decision more readable.
Every Mutant oxalate protocol starts with the same foundation:
This matters because oxalate patterns are easy to misread when the system is already overloaded.
If the user is underfed, over-supplemented, highly stressed, reacting to environmental triggers, or changing too many variables at once, the protocol becomes harder to interpret.
The foundation is not optional background.
It is what makes the protocol readable.
Mutant does not frame oxalate recovery as “just reintroduce oxalates.”
Some users may eventually broaden their diet, but that is not the protocol itself.
The protocol does not ask the user to challenge high-oxalate foods to prove recovery. It focuses on:
Food expansion, if it ever happens, is downstream of stability — not the starting goal.
Oxalobacter formigenes is often discussed in the oxalate community, but Mutant’s current oxalate protocols do not attempt to restore Oxalobacter or make it the central mechanism.
The Mutant roadmap focuses on mechanisms that can be more directly mapped into protocol decisions:
Oxalobacter may be biologically relevant in some contexts, but it is not the operational center of these protocols.
Because dietary oxalate is only one possible input.
A strict diet may lower external load, but it may not address sulfur-linked sensitivity, endogenous production, intestinal export failure, or enteric hyperabsorption from malabsorption.
Mutant helps identify which driver is most likely narrowing your threshold.
Not primarily.
The protocols are designed to avoid forced dumping and overshoot. The goal is not to trigger a purge. The goal is to stabilize the lane so your body’s response becomes more predictable and the next step is easier to judge.
If a protocol makes symptoms more chaotic, that is not automatically “progress.”
No.
Mutant provides educational analysis and protocol direction. It does not diagnose, treat, or cure disease.
The goal is to make the oxalate problem more organized: which driver fits, which supports are logical, which steps are risky, and when objective testing or medical evaluation matters.
A Calcium Anchor is the strategic use of calcium with an oxalate-containing meal to bind oxalate in the gut lumen before it is absorbed.
The key is timing.
Calcium taken away from food does not bind the oxalate in that meal.
This matters most in enteric hyperabsorption / malabsorption patterns.
B6, in its active PLP-related role, supports AGXT-dependent glyoxylate handling.
In the endogenous overproduction protocol, the goal is not megadosing. The protocol uses the concept of a low B6 adequacy floor and watches for response over time.
High-dose B6 belongs in a qualified hyperoxaluria evaluation context, not as a casual self-experiment.
B1 may be relevant to broader glyoxylate and energy metabolism, but it should not be presented as the main fix for every oxalate pattern.
In the current protocol set, B1 is not the central operational step. The endogenous production protocol focuses first on vitamin C exposure, B6 adequacy, binding/hydration signal protection, and objective urine testing.
Mutant supports two levels of genetic input:
Consumer DNA can be useful as a first pass, but it does not rule out rare or structural variants.
Whole genome sequencing can provide a more complete view when deeper resolution is needed.
Low-oxalate restriction can be useful as a temporary sanctuary.
It can lower exposure, reduce acute load, and help create a quieter baseline.
But restriction alone does not tell you which biological driver is narrowing your threshold.
Mutant’s approach is different:
The goal is not permanent restriction.
The goal is driver-matched stability.
Success does not have to mean eating high-oxalate foods.
Early success may look like:
A protocol is working when the system becomes more readable.
Stop self-directed protocol experimentation and seek formal evaluation when there are red flags such as:
Mutant is designed to help organize patterns, not replace evaluation for serious kidney, metabolic, or gastrointestinal conditions.
If you have been restricting oxalates for years and still feel reactive, the next step may not be another smaller food list.
It may be a clearer map.
Mutant helps identify which oxalate driver may be narrowing your threshold, then points you toward a protocol that fits that driver.
The goal is not to chase every oxalate theory.
The goal is to stop mixing lanes and start with the pattern most likely to matter.
Mutant provides educational, informational analysis and is not a substitute for medical advice, diagnosis, or treatment.