Quick Answer
Genetics often acts through systems, not isolated symptoms. A genetically stronger oxalate hub can still become unstable later if upstream hubs lose reserve first.
The clinical picture is often the result of an evolving loop between methylation, thyroid, histamine, and oxalates.
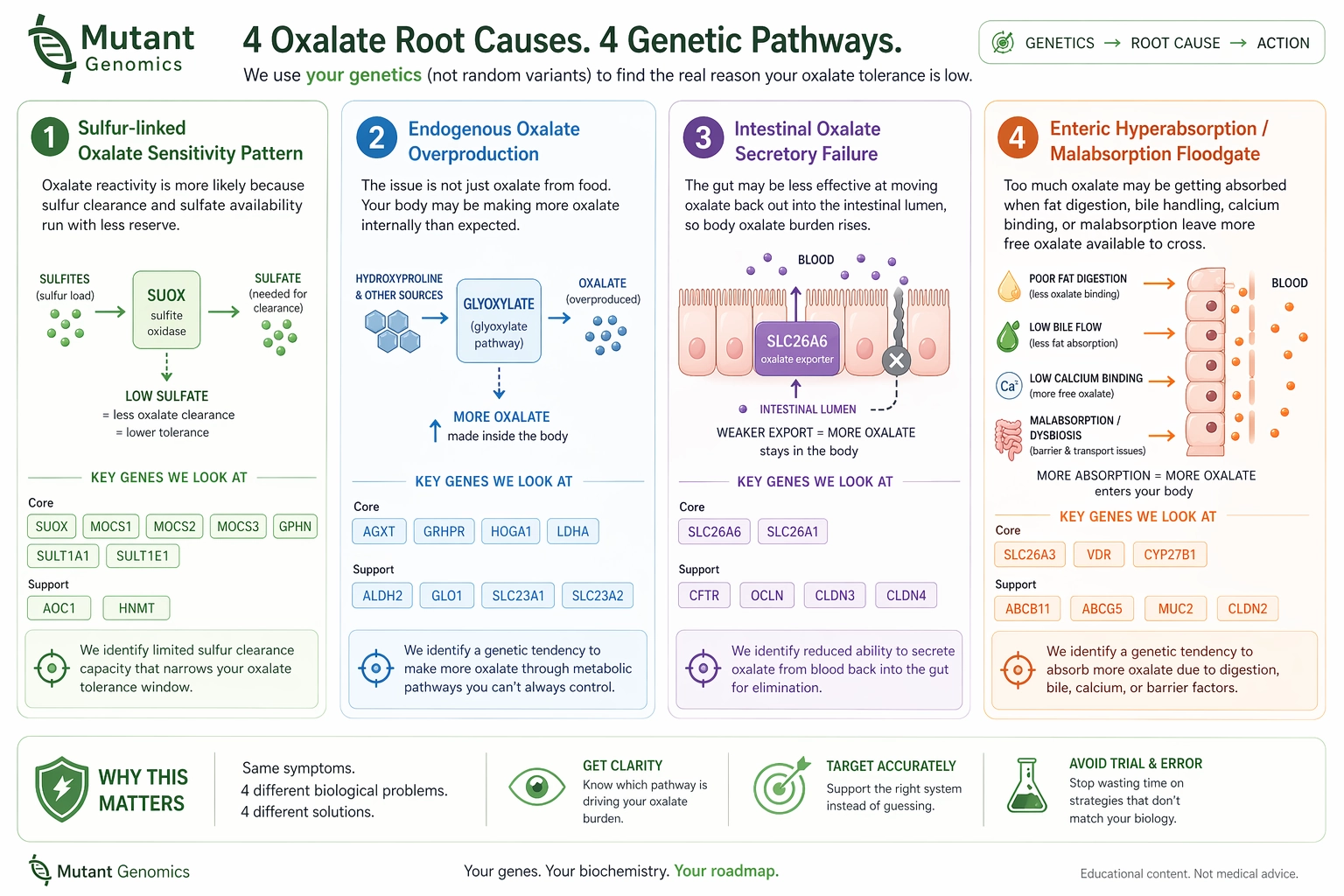
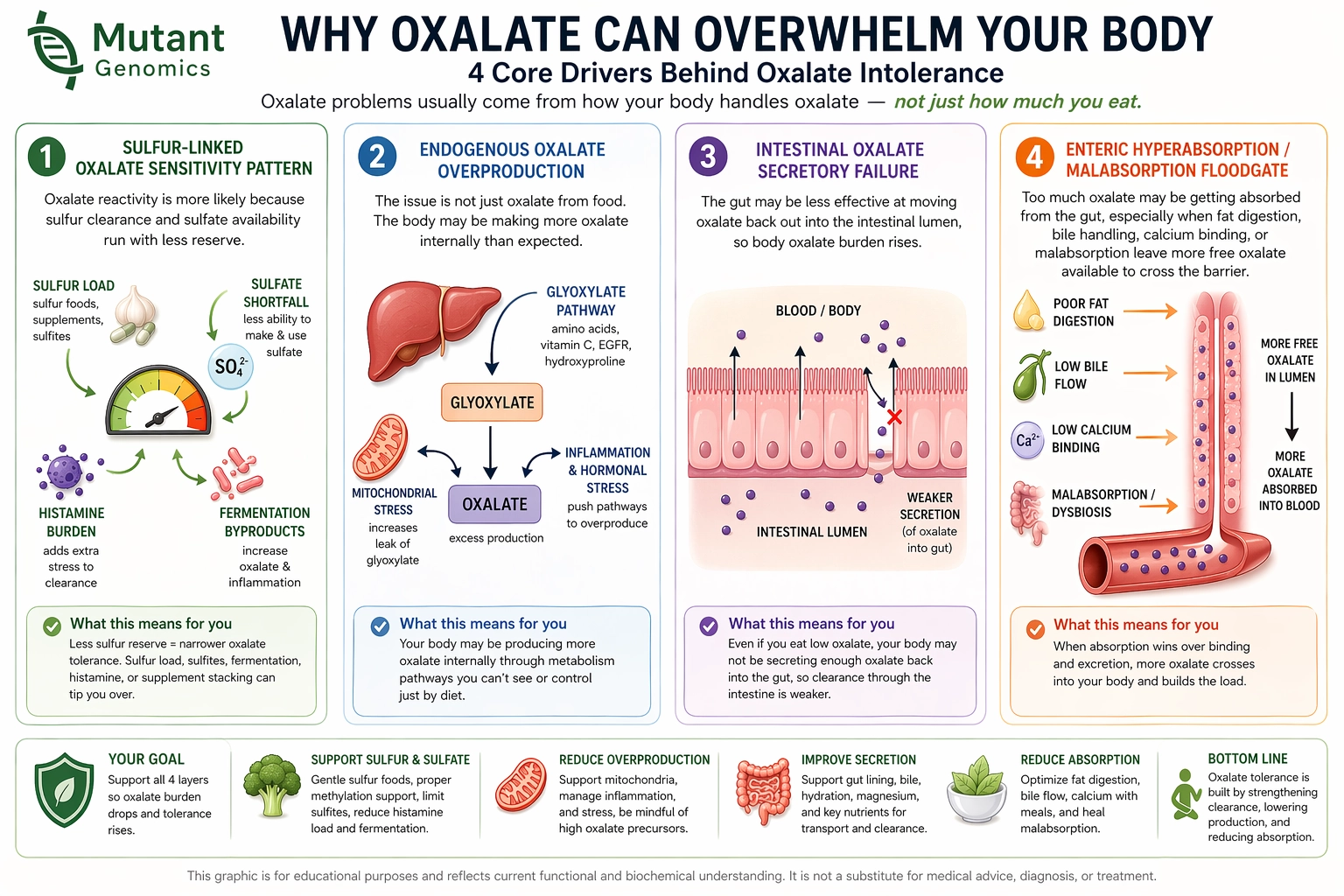
Mutant uses raw DNA data to map both the direct oxalate lanes and the upstream hubs that can quietly narrow tolerance over years.
- Use 23andMe or AncestryDNA for a first-pass oxalate stability map.
- Use WGS when you want broader genomic coverage and fewer blind spots.
- Use the roadmap to separate the loudest symptom from the most likely upstream driver.